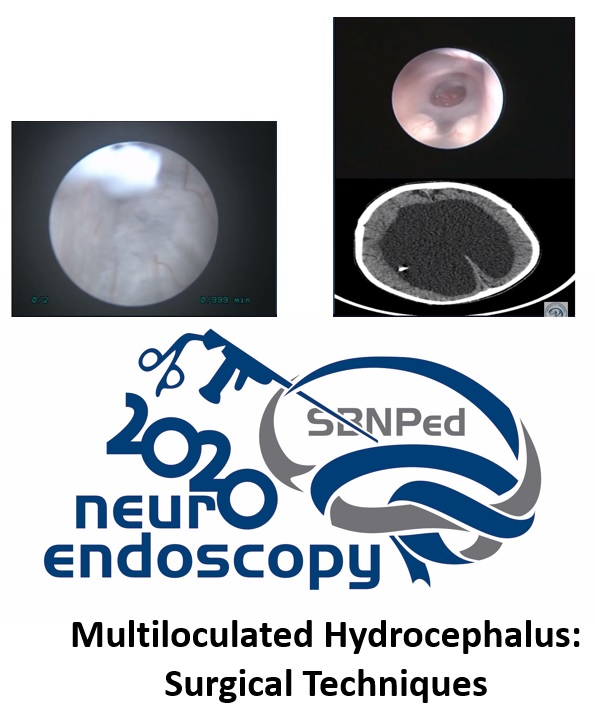
Multiloculated Hydrocephalus: Surgical Techniques
DOI:
https://doi.org/10.46900/apn.v3i1(January-April).72Keywords:
Hydrocep´halus, Multiloculated, Surgical TechniqueAbstract
Objective: Hydrocephalus shunt remains as the most common treatment choice for nonobstructive hydrocephalus, but in some cases multiloculated hydrocephalus (MH) remains a difficult neurosurgical disease despite of the different therapeutic options available. In children with MH multiple shunt procedures combined with neuroendoscopy may be required.(1) The rationale for neuroendoscopy in such complex cysts and multiloculated hydrocephalus is also to open several compartments to the normal fluid-filled spaces, minimize the number of isolated/loculated CSF spaces, and decrease shunt dependency and the number of proximal shunt catheters.(2) In such cases our major objective is keep the children with one or no one shunt and with one normal intracranial pressure (ICP).
Most patients with multiloculated hydrocephalus are infants with a severe disability who present with high intracranial pressure. Multiple shunting was a routine practice so far to normalize the intracranial pressure, but in these cases shunt complications could be quite common including shunt infection, malposition and malfunction which needed more shunt revision surgeries.(1, 3)
Neuroendoscopy has changed the treatment options for complex multiloculated hydrocephalus. The possibility to do several fenestrations and change multiples cysts in one simple cyst or ventricle was one important improvement in MH treatment.(4-6)
In this review we will discuss aspects related to etiology, surgical techniques, and results in multiloculated hydrocephalus.
Methods: The authors carried out a literature review on multiloculated hydrocephalus and evaluated a series of personal cases operated in the recent years.
The keywords loculated hydrocephalus and surgical technique were used in Pubmed database website. Fifty-two articles were obtained and reviewed. From these publications we select the most relevant ones for the presentation. The articles were divided according to the main subject, with articles on etiology, surgical techniques and outcomes were selected.
We also reviewed some difficult cases with MH from personal experience. In all of those cases endoscopy procedures were performed associated to shunt procedures in all cases. The authors described some different techniques of cyst fenestration and the association to shunt or not.
Results/Discussion: Neuroendoscopy has changed the treatment in MH. This is a very difficult and interesting disease. Common risk factors for the development of MH include intraventricular hemorrhage, bacterial meningitis, shunt infection, and cerebrospinal fluid (CSF) overdrainage from shunt placement (rare). The magnetic resonance imaging (MRI) or computerized tomography (CT) scan with evidence of septations causing marked nonuniform compartmentalization and enlargement within the ventricular system are the most important ways to do the diagnosis of MH. Predisposing factors include low birth weight, prematurity, perinatal complications, and congenital malformation.
Although the full pathogenesis of MLH remains unclear, it is known that inflammation leads to subependymal gliosis, which produces glial tufts and septations that occlude the normal ventricle system. Septations also develop via organization of intraventricular exudate and debris from ventriculitis.
Despite os clinical history of poor outcome, head circuference increase and prior infection or brain bleeding, we need image to perform the diagnosis. Types of loculated hydrocephalus could be divided in: multiloculated and uniloculated. The most important classification was done by Spennato.(5) He divided in five types:
1) hydrocephalus with multiple intraventricular septations;
2) isolated lateral ventricle/unilateral hydrocephalus;
3) entrapped temporal horn;
4) isolated fourth ventricle;
5) expanding cavum septi pellucidi/cavum vergae
Using the endoscope to treat MH has some advantages.(7, 8) This is a less invasiveness and this is very important in kids.(6) Avoidance of brain retraction, less blood loss, faster operation time, and shorter hospital stay. But endoscopy has some risk and possible complications. It also has several disadvantages. A subdural hematoma and/or hygroma may form, but the incidence of this is lower than with open craniotomy. The risk of ventriculitis, CSF leakage (subcutaneous CSF collection), and hemorrhage are reported to be like that with open craniotomy. Intraoperative bleeding can usually be easily managed by irrigation or coagulation. However, handling of significant intraoperative bleeding is not as easy in endoscopy as in open craniotomy.(9)
Some new technologies could improve the outcome and avoid risk and complications.(10, 11) Navigation could be used in two forms:
- Navigation system is used to planning the entry point and the endoscopy trajectory
- Endoscopy guided and navigation during all surgical time.
The evaluation of results is presented in different ways in the literature. The main outcomes observde for measuring results were: hydrocephalus control or not, number of surgery performed and number of catheters used.(4) Shunt Independence is rare.
Conclusion: Multiloculated hydrocephalus is one difficult disease to treat.(4) Neuroendoscopy cyst fenestration was one great improvement in treatment of MH, but after this new procedure the clinical outcome still no so good. Endoscopy is important to decrease the number of shunts and surgeries.
Downloads
References
Deopujari CE, Padayachy L, Azmi A, Figaji A, Samantray SK. Neuroendoscopy for post-infective hydrocephalus in children. Childs Nerv Syst. 2018;34(10):1905-14.
Warf BC, Campbell JW, Riddle E. Initial experience with combined endoscopic third ventriculostomy and choroid plexus cauterization for post-hemorrhagic hydrocephalus of prematurity: the importance of prepontine cistern status and the predictive value of FIESTA MRI imaging. Childs Nerv Syst. 2011;27(7):1063-71.
Zandian A, Haffner M, Johnson J, Rozzelle CJ, Tubbs RS, Loukas M. Endoscopic third ventriculostomy with/without choroid plexus cauterization for hydrocephalus due to hemorrhage, infection, Dandy-Walker malformation, and neural tube defect: a meta-analysis. Childs Nerv Syst. 2014;30(4):571-8.
Zuccaro G, Ramos JG. Multiloculated hydrocephalus. Childs Nerv Syst. 2011;27(10):1609-19.
Spennato P, Cinalli G, Ruggiero C, Aliberti F, Trischitta V, Cianciulli E, et al. Neuroendoscopic treatment of multiloculated hydrocephalus in children. J Neurosurg. 2007;106(1 Suppl):29-35.
Cinalli G, Cappabianca P, de Falco R, Spennato P, Cianciulli E, Cavallo LM, et al. Current state and future development of intracranial neuroendoscopic surgery. Expert Rev Med Devices. 2005;2(3):351-73.
Cinalli G, Peretta P, Spennato P, Savarese L, Varone A, Vedova P, et al. Neuroendoscopic management of interhemispheric cysts in children. J Neurosurg. 2006;105(3 Suppl):194-202.
Di Rocco C, Cinalli G, Massimi L, Spennato P, Cianciulli E, Tamburrini G. Endoscopic third ventriculostomy in the treatment of hydrocephalus in pediatric patients. Adv Tech Stand Neurosurg. 2006;31:119-219.
Akbari SH, Limbrick DD, Kim DH, Narayan P, Leonard JR, Smyth MD, et al. Surgical management of symptomatic Chiari II malformation in infants and children. Childs Nerv Syst. 2013;29(7):1143-54.
Kim SA, Letyagin GV, Danilin VE, Sysoeva AA, Rzaev JA, Moisak GI. The benefits of navigated neuroendoscopy in children with multiloculated hydrocephalus. Asian J Neurosurg. 2017;12(3):483-8.
Piyachon S, Wittayanakorn N, Kittisangvara L, Tadadontip P. Treatment of multi-loculated hydrocephalus using endoscopic cyst fenestration and endoscopic guided VP shunt insertion. Childs Nerv Syst. 2019;35(3):493-9.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2021 Ricardo de Amoreira Gepp

This work is licensed under a Creative Commons Attribution 4.0 International License.

When publishing in Archives of Pediatric Neurosurgery journal, authors retain the copyright of their article and agree to license their work using a Creative Commons Attribution 4.0 International Public License (CC BY 4.0), thereby accepting the terms and conditions of this license (https://creativecommons.org/licenses/by/4.0/legalcode).
The CC BY 4.0 license terms applies to both readers and the publisher and allows them to: share (copy and redistribute in any medium or format) and adapt (remix, transform, and build upon) the article for any purpose, even commercially, provided that appropriate credit is given to the authors and the journal in which the article was published.
Authors grant Archives of Pediatric Neurosurgery the right to first publish the article and identify itself as the original publisher. Under the terms of the CC BY 4.0 license, authors allow the journal to distribute the article in third party databases, as long as its original authors and citation details are identified.